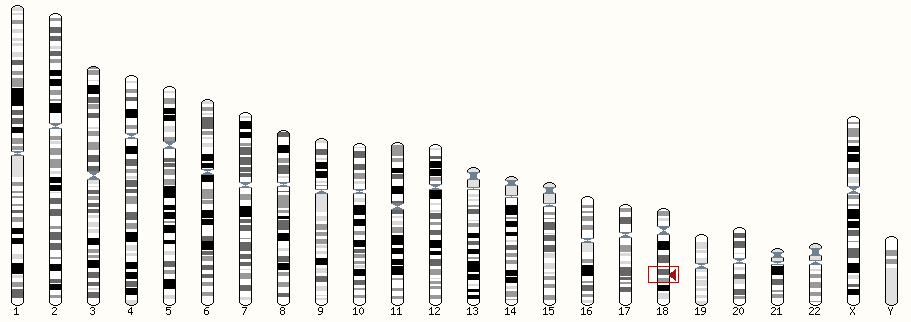
Pitt-Hopkins syndrome (PTHS) is caused by changes in the TCF4 gene on chromosome 18.
Genes are like instruction booklets that tell the cells in our bodies how to make proteins. We have two copies of every gene – one from our mother, one from our father. Variations change the DNA code of genes so that they cannot make a proper protein.
Children with PTHS have a change in one copy their tcf4 gene so that it no longer codes for a TCF4 protein. The brain cannot develop properly without both working copies of tcf4
In most cases, there is no family history of PTHS and the child is the first person in the family to have the change in the TCF4 gene. Doctors call this a ‘de novo’ variation. De novo variations usually arise in the mother’s egg, the father’s sperm or very early in the child’s embryonic development. This means that the chance of having another child with PTHS is low.
More than one child with PTHS in a family has been reported in 4 instances of published cases. This probably happened because one parent had the change in several egg or sperm cells. This is called mosaicism and the chances of this happening are thought to be about 2%.
If you have a child with PTHS and are having another baby, you can ask for genetic testing while you are pregnant to see if your new baby has PTHS. The lab will check your new baby’s DNA for the same mutation that your child with PTHS has.
TCF4 mutations cannot be found in a small proportion of children who have PTHS symptoms. There are several possible reasons for this:
- The child has an unusual type of change that we are unable to see with existing gene testing techniques
- There is a second, unknown, gene that causes PTHS
Even if no change in the TCF4 is found, if the child has symptoms of PTHS then a diagnosis can be made. If a diagnosis is made based on symptoms, it is called a clinical diagnosis. Healthy siblings of people with PTHS have no risk of being mosaic, so are at no increased risk of having a child with PTHS.
There are two syndromes that are very similar to PTHS but are even rarer and caused by different genes. They are called Pitt-Hopkins-like syndrome 1 (PTHSL1) and Pitt-Hopkins-like syndrome 2 (PTHSL2).
PTHSL1 is caused by mutations in the CNTNAP2 gene on chromosome 7.
PTHSL2 is caused by mutations in the NRXN1 gene on chromosome 2.
PTHSL1 and 2 are both recessively inherited, meaning that the child has mutations in both copies of CNTNAP2 or NRXN1 and both parents are carriers, each having one mutation. In these families, there is a 1 in 4 chance of having another child with PTHSL1 or 2.
Literature
De Pontual L, et al. Mutational, functional, and expression studies of the TCF4 gene in Pitt-Hopkins syndrome. Hum Mutat 2009;30:669-76.
Giurgea I, et al. TCF4 deletions in Pitt-Hopkins Syndrome. Hum Mutat 2008;29: E242-51.
Kalscheuer VM, et al. Disruption of the TCF4 gene in a girl with mental retardation but without the classical Pitt-Hopkins syndrome. Am J Med Genet 2008;146A:2053-9.
Kim SK, et al. CpG methylation in exon 1 of transcription factor 4 increases with age in normal gastric mucosa and is associated with gene silencing in intestinal-type gastric cancers. Carcinogenesis 2008;29:1623-31.
Ouvrier R. Hyperventilation and the Pitt-Hopkins syndrome. Dev Med Child Neurol 2008;50:481.
Zweier C, et al. Further delineation of Pitt-Hopkins syndrome: phenotypic and genotypic description of 16 novel patients. J Med Genet 2008;45:738-44.
Zweier C, et al. CNTNAP2 and NRXN1 are mutated in autosomal recessive Pitt-Hopkins-like mental retardation and determine the level of a common synaptic protein in Drosophila. Am J Hum Genet 2009;85:655-66.
Zollino.M et al. Clinical Genetics. 2019;95:462–478.Diagnosis and management in Pitt-Hopkins syndrome: First international consensus statement Clinical Genetics. 2019;95:462–478.